{kind=link}
This review offers an in-depth exploration of Nodular Lymphocyte Predominant Hodgkin Lymphoma (NLPHL), highlighting its distinct characteristics across various domains such as epidemiology, clinical presentation, histopathology, immunophenotype, genetic findings, and challenges in differential diagnosis.

Credit: Elaine S. Jaffe, Yanna Ding
This review offers an in-depth exploration of Nodular Lymphocyte Predominant Hodgkin Lymphoma (NLPHL), highlighting its distinct characteristics across various domains such as epidemiology, clinical presentation, histopathology, immunophenotype, genetic findings, and challenges in differential diagnosis.
Epidemiology and Clinical Presentation
NLPHL is a relatively rare subtype of Hodgkin lymphoma, comprising approximately 10% of all Hodgkin lymphoma cases. It predominantly affects males, with a higher incidence observed in those aged 30 to 50 years. Unlike classical Hodgkin lymphoma, NLPHL often presents with localized lymphadenopathy rather than systemic symptoms, which are rare unless the disease is in an advanced stage. The most commonly involved sites include the cervical, axillary, and inguinal lymph nodes, with mediastinal and extranodal presentations being less frequent. The disease generally follows an indolent course, but in approximately 5-10% of cases, it can transform into diffuse large B-cell lymphoma (DLBCL), which has a more aggressive clinical course.
Histopathologic Characteristics
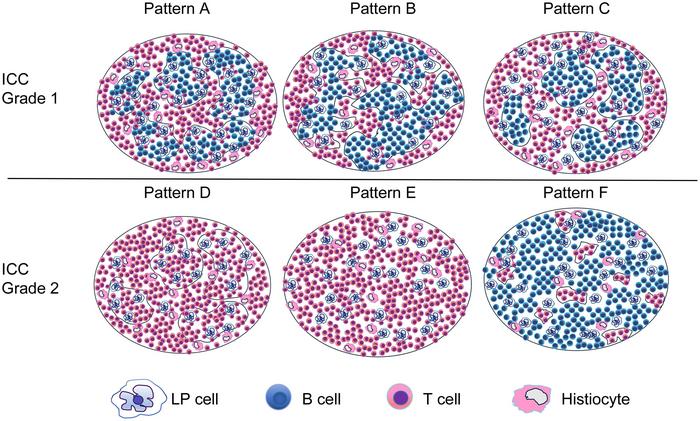
NLPHL is characterized histologically by a nodular growth pattern, often involving pre-existing reactive follicles. The hallmark cells of NLPHL are the lymphocyte-predominant (LP) cells, also known as “popcorn cells” due to their distinctive multilobated nuclei. These cells are typically surrounded by a background of small lymphocytes and histiocytes. A notable feature in NLPHL is the presence of progressive transformation of germinal centers (PTGC), which can be observed in the surrounding non-involved lymphoid tissue. However, PTGC is not considered a direct precursor to NLPHL, and its presence does not necessarily increase the risk of developing the disease.
Immunophenotype
The immunophenotypic profile of NLPHL is distinct, with LP cells expressing B-cell markers such as CD20, CD79a, Pax5, and Bcl-6. Notably, these cells lack expression of CD10 and MUM-1/IRF4, which are commonly found in other types of lymphoma. The LP cells show strong expression of transcription factors Oct-2 and Bob1, which are crucial for immunoglobulin transcription. Furthermore, LP cells in NLPHL are generally negative for Epstein-Barr virus (EBV), distinguishing them from certain subtypes of classical Hodgkin lymphoma where EBV is frequently detected. An intriguing aspect of NLPHL is the presence of T-follicular helper (TFH) cells, which form rosettes around the LP cells and may play a role in the pathogenesis of the disease.
Genetic Findings
Genetic studies of NLPHL reveal that the LP cells carry functional immunoglobulin rearrangements and exhibit a high load of somatic hypermutations, indicative of their origin from germinal center B-cells. Mutations in genes such as PAX5, PIM1, RHOH, and MYC have been identified, alongside aberrations in SGK1, DUSP2, and JUNB. These genetic features highlight the complexity of NLPHL and suggest a close relationship with T-cell/histiocyte-rich large B-cell lymphoma (THRLBL), another type of lymphoma that shares some histologic and immunophenotypic similarities with NLPHL.
Differential Diagnosis
The differential diagnosis of NLPHL is challenging due to its overlapping features with other lymphomas, particularly THRLBL and lymphocyte-rich classical Hodgkin lymphoma (LRCHL). While NLPHL and THRLBL share several genetic and immunophenotypic characteristics, they differ in clinical presentation and histopathologic features. THRLBL often presents with more widespread disease and systemic symptoms, whereas NLPHL typically remains localized with an indolent course. Histologically, NLPHL can be distinguished from LRCHL by its nodular growth pattern and the presence of LP cells. In contrast, LRCHL is characterized by regressed germinal centers and a distinct mantle zone, which are not features of NLPHL.
Conclusions
The review underscores the importance of recognizing the diverse histopathologic and immunophenotypic features of NLPHL for accurate diagnosis and treatment. The close relationship between NLPHL and other lymphomas, such as THRLBL, necessitates careful consideration in differential diagnosis to avoid misclassification. Understanding the unique characteristics of NLPHL, including its epidemiology, clinical presentation, and genetic underpinnings, is crucial for developing effective therapeutic strategies and improving patient outcomes.
Full text
The study was recently published in the Journal of Clinical and Translational Pathology.
Journal of Clinical and Translational Pathology (JCTP) is the official scientific journal of the Chinese American Pathologists Association (CAPA). It publishes high quality peer-reviewed original research, reviews, perspectives, commentaries, and letters that are pertinent to clinical and translational pathology, including but not limited to anatomic pathology and clinical pathology. Basic scientific research on pathogenesis of diseases as well as application of pathology-related diagnostic techniques or methodologies also fit the scope of the JCTP.
Follow us on X: @xiahepublishing
Follow us on LinkedIn: Xia & He Publishing Inc.
Journal
Journal of Clinical and Translational Pathology
Article Title
Histopathologic Features and Differential Diagnosis in Challenging Cases of Nodular Lymphocyte Predominant B-cell Lymphoma/Nodular Lymphocyte Predominant Hodgkin Lymphoma
Article Publication Date
17-Jun-2024