
Health care providers can more effectively connect parents and other caregivers of children to needed social resources when they present a menu of options rather than using standard screening tools, a recent study found. The research will be presented at the Pediatric Academic Societies (PAS) 2024 Meeting, held May 3-6 in Toronto.
Health care providers can more effectively connect parents and other caregivers of children to needed social resources when they present a menu of options rather than using standard screening tools, a recent study found. The research will be presented at the Pediatric Academic Societies (PAS) 2024 Meeting, held May 3-6 in Toronto.
According to researchers at the Children’s Hospital of Philadelphia, health care providers typically use risk-based screening to identify families facing food and housing insecurity, financial strain, and unsafe environments. Experts say this approach can lead to inequalities in resource distribution and usage by requiring families to disclose hardships—often in front of their children—in order to receive assistance. Researchers found that allowing family members to select desired resources from a menu of options increased the interest in and use of social support.
Researchers randomly provided nearly 4,000 caregivers with either a traditional social risk screening tool, a resource menu, or no assessment. Participants using the resource menu were 9.4% more likely to request resources than those using the screening tool, the study found. The beneficial effect of the resource menu was even more pronounced among families who prefer a non-English language. More than 40% of the participants used an online resource map to access resources, while 33.4% reported sharing it.
“Children and families with social need should receive resources that reflect their priorities, not based on whether they meet the threshold of a screening tool,” said Danielle Cullen, MD, MPH, MSHP, assistant professor at Children’s Hospital of Philadelphia and presenting author. “Using a ‘resource menu’ allows for a more family-centered approach to resource connection, equipping children and families with tailored social resources based on their priorities while reducing inequalities and feared unintended consequences that may be perpetuated by screening practices.”
Study authors recommend that providers use resource menus as an alternative to social risk screening to provide a more equitable, family-centered approach.
# # #
EDITOR:
Dr. Danielle Cullen will present “Socially Equitable Care by Understanding Resource Engagement (SECURE): A Pragmatic RCT” on Saturday, May 4 from 8:15-8:30 AM E.T.
Reporters interested in an interview with Dr. Cullen should contact Amber Fraley at amber.fraley@pasmeeting.org.
The PAS Meeting connects thousands of pediatricians and other health care providers worldwide. For more information, please visit www.pas-meeting.org.
About the Pediatric Academic Societies Meeting
Pediatric Academic Societies (PAS) Meeting connects thousands of leading pediatric researchers, clinicians, and medical educators worldwide united by a common mission: Connecting the global academic pediatric community to advance scientific discovery and promote innovation in child and adolescent health. The PAS Meeting is produced through the partnership of four leading pediatric associations; the American Academy of Pediatrics (AAP), the Academic Pediatric Association (APA), the American Pediatric Society (APS), and the Society for Pediatric Research (SPR). For more information, please visit www.pas-meeting.org. Follow us on X @PASMeeting and like us on Facebook PASMeeting.
Abstract: Socially Equitable Care by Understanding Resource Engagement (SECURE): A Pragmatic RCT
Presenting Author: Danielle Cullen, MD, MPH, MSHP
Organization
Children’s Hospital of Philadelphia
Topic
Health Equity/Social Determinants of Health
Background
Despite the increase in social risk screening protocols across healthcare, growing evidence suggests that patient interest in resources does not necessarily correlate with a positive screen, and that screening may limit acceptance of resources due to fear of stigma or negative repercussion. Identifying an alternative to the standard deficits-based screening process, such as a resource menu where caregivers self-select from a list of resource domains without prerequisite disclosure of risk, may be a key lever to improve connection with desired resources.
Objective
This study compares caregivers’ acceptance of and engagement with social resource information when that information is 1) presented alone, 2) following a resource menu, or 3) following standardized social risk screening.
Design/Methods
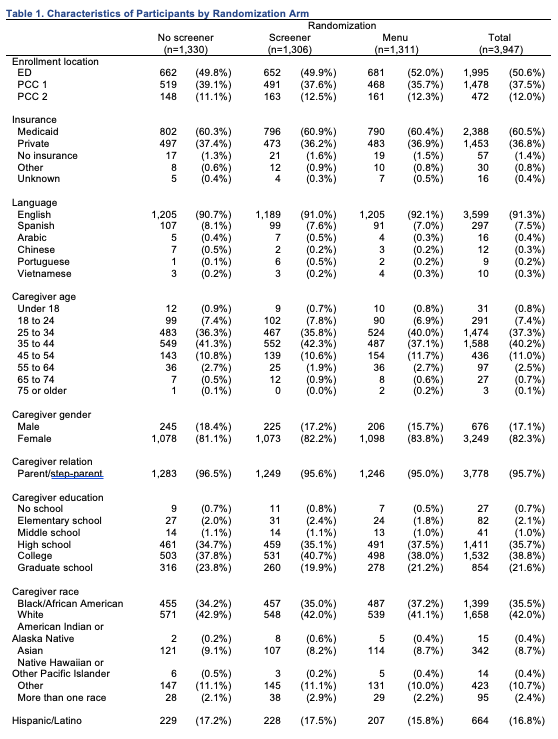
In this 3-arm pragmatic RCT, we recruited adult caregivers of pediatric patients in the Emergency Department and 2 primary care clinics associated with a freestanding children’s hospital. Caregivers speaking any of the 6 study languages were randomized to 1) an evidence-based social risk screener, 2) a resource menu, or 3) no assessment. All caregivers were provided with an electronic resource map, individual resource navigation 5 days after enrollment, and could request a same-day social work consultation; automatic same-day consultation was triggered for any emergent needs identified by screening. Consenting caregivers were contacted with a survey 30 days after enrollment to assess reported use of the resource map. Between group differences were assessed with the Chi-squared test and logistic regression.
Results
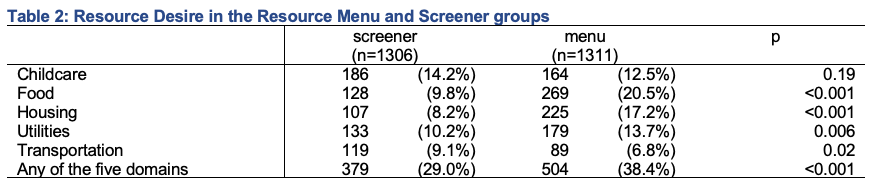
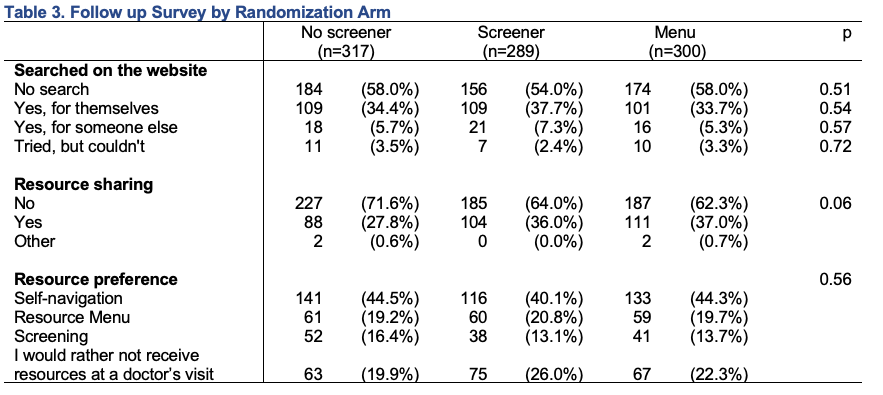
Among the 3,947 participants randomized, 2,636 (66.8%) reported prior use of a social resource. A significantly higher proportion of participants in the resource menu arm reported desire for resources compared to the screening arm (38.4% vs 29.0%, P< 0.001). Among the 906 follow-up survey participants, 40.2% reported using the resource map, and 33.4% reported sharing the resource map. There were no significant differences between randomization arms in terms of rate or domains of reported searches.
Conclusion(s)
Our results suggest that healthcare providers can better recognize their patients’ desire for social resources using a “resource menu” – focusing on caregiver prioritized domains of social need – rather than screening for areas of social risk. This allows for a more family-centered approach to resource connection. Further analysis will assess the impact of randomization arm on how families search data from the resource map, engage with resource navigation, and report change in social risk.
Tables and Images
Article Title
Socially Equitable Care by Understanding Resource Engagement (SECURE): A Pragmatic RCT

{kind=link}
{kind=link}
{kind=link}
{kind=link}